

Breakthrough in glioma treatment: from the intracranial black box to precise targeting, multi-path breakthroughs rewrite patients fate
Glioblastoma (GBM) is the most common and aggressive primary brain tumor, with a median survival of only 12-21 months and a 5-year survival rate of less than 5%. For a long time, the blood-brain barrier blocking drug penetration, the high heterogeneity of the tumor, and the immunosuppressive microenvironment have made gliomas the most difficult 'intracranial fortress' to conquer. However, with the rapid development of oncolytic viruses, targeted drugs, gene therapy, and physical methods to open the blood-brain barrier, glioma treatment is ushering in a historic turning point from 'passive resistance' to 'active breakthrough.'

Mechanistic Breakthrough: Breaking the 'Self-Built High Wall' and Immune Evasion of Gliomas
The resistance of gliomas to treatment not only arises from the physical barrier of the blood-brain barrier but also from the complex defensive system constructed by the tumor itself. In 2025, Academician Zhou Liangfu and Professor Shi Zhifeng's team at Huashan Hospital affiliated with Fudan University published a significant study in *Neuro-Oncology*, revealing for the first time the 'Tumor Self-Rampart' resistance mechanism of gliomas under the pressure of oncolytic virus therapy.
The research team established an innovative RESCUE translational research framework and used patient-derived xenograft (PDX) models to 'replicate' the clinical treatment process. They found that after oncolytic adenovirus infects tumor cells, it activates the BCL10 gene, which in turn induces paracrine secretion of the cytokine IL-8 through the NF-κB signaling pathway. IL-8 further induces nearby uninfected tumor cells to enter senescence prematurely. These senescent cells accumulate around necrotic areas, forming a highly fibrotic physical barrier, while the virus replication ability of the senescent cells significantly decreases, creating a biological barrier. This dual barrier greatly blocks the spread of the virus within glioma tissue, resulting in the 'waning effectiveness' of oncolytic virus therapy.
Through whole-genome CRISPR screening and spatial transcriptomics analysis, the research team precisely pinpointed IL-8 as the core target and screened the IL-8 receptor-targeting inhibitor Raperixin. When combined with oncolytic viruses, it can effectively inhibit the formation of isolation bands and significantly enhance viral replication efficiency. Even more unexpectedly, the study found that early use of glucocorticoids not only does not affect efficacy due to immunosuppression, but instead can eliminate IL-8-driven isolation band formation through anti-inflammatory effects, providing important guidance for precise clinical medication.
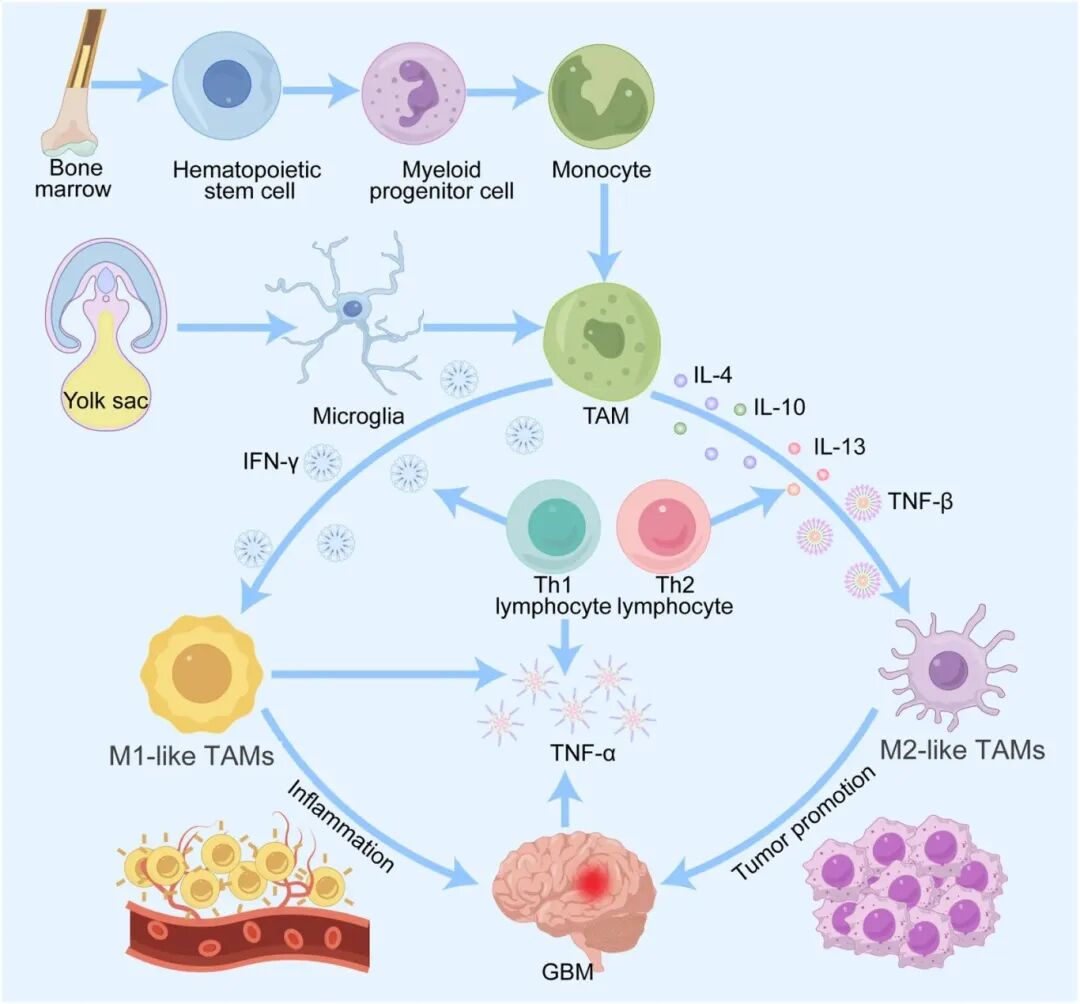
Meanwhile, the role of tumor-associated macrophages (TAMs) in glioma immune evasion has also been deeply analyzed. TAMs account for 30%-50% of the total glioma tumor mass, and their M2-polarized subpopulation forms a potent immunosuppressive barrier by secreting immunosuppressive factors such as TGF-β and IL-10, and by upregulating PD-L1 expression. A 2025 review in *Frontiers in Cell and Developmental Biology* systematically summarized five major mechanisms by which TAMs mediate chemotherapy resistance: regulation of drug-metabolizing enzymes, secretion of pro-tumor factors, maintenance of glioma stem cell stemness through interactions, adaptation to hypoxic microenvironments, and remodeling of the extracellular matrix via matrix metalloproteinases (MMPs) to increase tissue stiffness, thereby hindering drug penetration. These findings lay the theoretical foundation for therapeutic strategies targeting TAMs.
Innovation in Treatment Strategies: From 'Passive Defense' to 'Active Breakthrough'
(1) Physical Barrier Disruption: Focused Ultrasound Opens the Blood-Brain Barrier
The blood-brain barrier is the core obstacle for drug delivery in gliomas. The BT008NA multicenter Phase I/II trial, published in The Lancet Oncology in 2025, confirmed for the first time in humans the safety and feasibility of microbubble-enhanced focused ultrasound (MB-FUS) combined with temozolomide in the treatment of high-grade gliomas.
The study included 34 patients with newly diagnosed high-grade gliomas. During six cycles of temozolomide chemotherapy, MB-FUS treatment was performed within the first three days of each cycle to precisely open the blood-brain barrier in tumor-infiltrated regions. The results showed that all treatments successfully opened the blood-brain barrier, with no treatment-related deaths. The median overall survival of patients reached 31.3 months, and the median progression-free survival was 13.5 months, significantly longer than historical data. Even more encouragingly, changes in plasma free DNA levels after MB-FUS treatment closely corresponded to patient disease courses, suggesting that this technology could also be used for 'acoustic liquid biopsy' to achieve non-invasive dynamic monitoring. This technology provides a physical pathway for chemotherapy drugs and subsequent immunotherapy to enter the brain, with broad prospects for combined applications.
(2) Precise Targeting: Milestone Breakthrough of IDH1 Mutation Inhibitors
IDH1 mutations are key driver genes in low-grade gliomas and some high-grade gliomas. In February 2026, Nuvation Bio announced the official launch of its global Phase III SIGMA trial (G203) for Safusidenib, an oral, highly brain-penetrant mutant IDH1 inhibitor, marking a decisive step towards clinical translation of this target.

Safusidenib has demonstrated good tolerability and anti-tumor activity in Phase I/II clinical trials. This Phase III trial will include approximately 300 patients with IDH1-mutant astrocytoma (including high-risk grade 2, grade 3, and grade 4), with the primary endpoint being progression-free survival (PFS) assessed by blinded independent central review. At the same time, the trial has added an exploratory cohort of approximately 40 patients with grade 3 oligodendroglioma to evaluate the objective response rate in patients who have not received radiotherapy or chemotherapy. David Arons, President of the National Brain Tumor Society in the United States, pointed out: 'Patients with IDH1-mutant gliomas have long lacked proven survival-extending treatments, and this registrational trial is expected to bring breakthroughs to this highly unmet need area.'
(3) Immune double anti-DNA drugs: synergistically activating anti-tumor immunity
In March 2026, Akeso Bio reached a cooperation agreement with INOVIO to jointly explore an innovative approach for treating glioblastoma using the world's first PD-1/CTLA-4 bispecific antibody cadonilimab in combination with the DNA drug INO-5412. This combination therapy has been included in the INSIGhT Phase II adaptive platform trial initiated by Dana-Farber Cancer Institute.

INO-5412 encodes three high-priority tumor antigens: hTERT, WT1, and PSMA, and also encodes IL-12 to activate T cell immune responses. Previous Phase II studies have shown that INO-5412 combined with PD-1 inhibitors can induce strong antigen-specific T cell responses and promote T cell infiltration into the tumor microenvironment. Cadonilimab, as the world's first approved PD-1/CTLA-4 bispecific antibody, can simultaneously block two immune checkpoints, theoretically producing a synergistic effect. David Reardon, director of the Dana-Farber Neuro-Oncology Center, stated: 'Glioblastoma is one of the malignant tumors with the least effective treatment options at present, and this innovative immunotherapy combination may overcome challenges that single checkpoint inhibitors find difficult to address.'
(4) Breaking New Ground in Gene Therapy: AAV Vector Receives First FDA IND Approval
In February 2026, Siren Biotechnology announced that its AAV-based immunogene therapy SRN-101 received FDA approval for a new drug clinical trial (IND) to treat recurrent high-grade glioma. This is the first time the FDA has approved an AAV vector for a tumor indication, marking a significant breakthrough for gene therapy in the field of solid tumors.
SRN-101 uses a recombinant AAV vector to deliver engineered immune-modulating genes directly to the tumor microenvironment, aiming to trigger a durable anti-tumor immune response. Preclinical studies have shown that this therapy has potent anti-tumor activity in brain cancer models. The approval of this IND paves the way for the application of gene therapy in the field of brain tumors and also provides a new platform for subsequent combination therapies.
(5) Targeting the Microenvironment: From Macrophages to Oxidative Stress
Intervention strategies targeting the tumor microenvironment are also progressing rapidly. Various strategies targeting TAMs have entered preclinical and early clinical stages: CCR2 inhibitors can block the infiltration of monocytes into tumors; CSF1R inhibitors can deplete M2 macrophages; blocking the CD47-SIRPα axis restores the phagocytic function of TAMs against tumor cells. In addition, in March 2026, Professor Ester Hammond's team at the University of Oxford received funding from Brain Research UK to conduct research on Ag5 combined with radiotherapy for treating pediatric high-grade gliomas. Ag5 is a silver atom cluster compound that selectively increases reactive oxygen species (ROS) levels in tumor cells, pushing them beyond the tolerance threshold to induce cell death, while producing a synergistic killing effect when combined with radiotherapy.

Outlook: From Single-Point Breakthrough to Systemic Change
Current glioma research has developed a multidimensional treatment framework of 'physical barrier opening—precise targeted driving—immune synergistic activation—microenvironment remodeling.' Focused ultrasound opens physical channels for drug entry; IDH1 inhibitors provide precise targeting for specific mutation populations; oncolytic viruses combined with immunotherapy break through the limitations of 'cold tumors'; AAV gene therapy opens new therapeutic paradigms. In the future, with further integration of multi-omics screening, spatial transcriptomics, and personalized medication, combination treatment strategies based on patients' tumor mutation profiles and microenvironment characteristics will gradually be implemented.
It is foreseeable that glioma treatment is shifting from the traditional paradigm of 'surgery, radiotherapy, and chemotherapy' to a systematic transformation of 'physical barrier disruption, precise targeting, immune activation, and genetic modification.' This is not just an enrichment of therapeutic methods but also a subversion of the concept of 'incurable intracranial disease.' With more phase III clinical trial data emerging, the hope for long-term survival in glioma patients is moving from vision to reality.