

Merck Acquires Verona Pharma: How Can Animal Models Empower COPD Drug Development?
On July 9, American pharmaceutical giant Merck announced that it would acquire the UK biopharmaceutical company Verona Pharma, which focuses on respiratory diseases, for about $10 billion.
Through this acquisition, Merck will gain Verona Pharma's chronic obstructive pulmonary disease (COPD) treatment drug Ohtuvayre™ (brand name: Ensifentrine), enhancing its pipeline of COPD therapies.
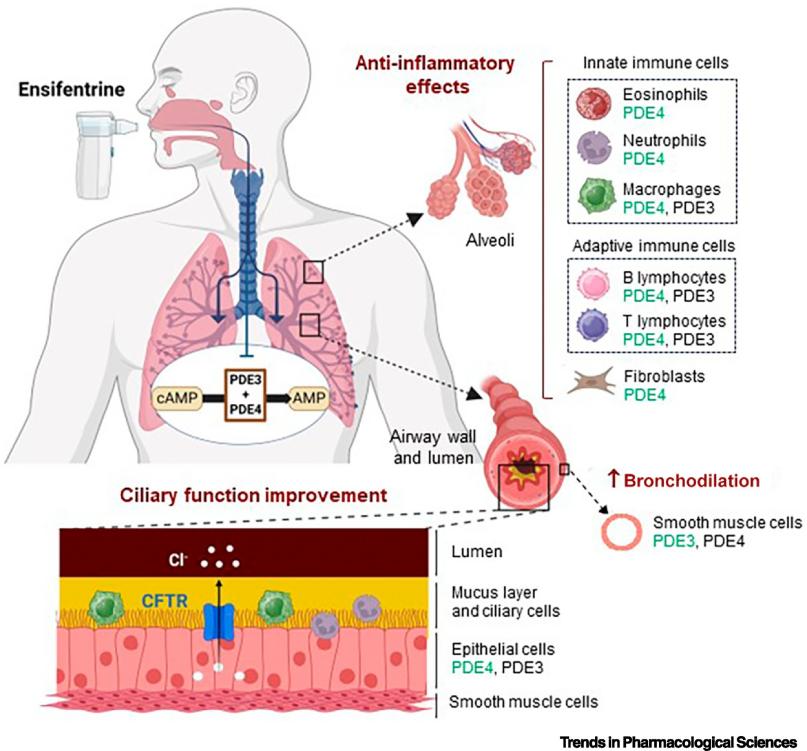
Ensifentrine is a first-in-class selective dual inhibitor of phosphodiesterase 3 and 4 (PDE3 and PDE4). It elevates cAMP by inhibiting PDE3, relaxing airway smooth muscle, while simultaneously inhibiting PDE4 to reduce inflammatory cell activation and migration, providing both bronchodilator and non-steroidal anti-inflammatory effects.
It is used for the maintenance treatment of chronic obstructive pulmonary disease (COPD) in adults. The drug was approved by the U.S. Food and Drug Administration (FDA) in June 2024, marking the first new inhalation mechanism therapy for COPD in over twenty years. Currently, it is also being evaluated in clinical trials for the treatment of non-cystic fibrosis bronchiectasis. Forecasts indicate that by the mid-2030s, annual sales of this drug could reach nearly $4 billion.
Chronic Obstructive Pulmonary Disease (COPD), often simply referred to as chronic bronchitis and emphysema, is a heterogeneous lung disease characterized by chronic respiratory symptoms (such as dyspnea, coughing, sputum production, and/or exacerbations) caused by airway abnormalities (bronchitis, bronchiolitis) and/or alveolar abnormalities (emphysema), leading to persistent and usually progressive airflow limitation.
The most common cause is cigarette smoke, while other risk factors include exposure to occupational dust and chemicals, air pollution, and genetic factors (such as alpha-1 antitrypsin deficiency).
According to WHO data, COPD is the fourth leading cause of death worldwide, causing 3.5 million deaths in 2021, accounting for approximately 5% of global deaths.
Due to the combined effects of continued exposure to risk factors and the aging global population, the prevalence and burden of COPD are expected to continue increasing in the coming decades.
As a chronic respiratory disease of national concern, COPD has been identified as a key focus of prevention and treatment in the "Healthy China 2030" action plan, and in September 2024, it was included in the national basic public health services program, indicating a substantial demand for medication in its market.
The pathogenesis of COPD is not yet fully understood. Chronic airway inflammation, oxidative stress, and protease/antiprotease imbalance-induced lung tissue damage are key factors in the pathogenesis of COPD.
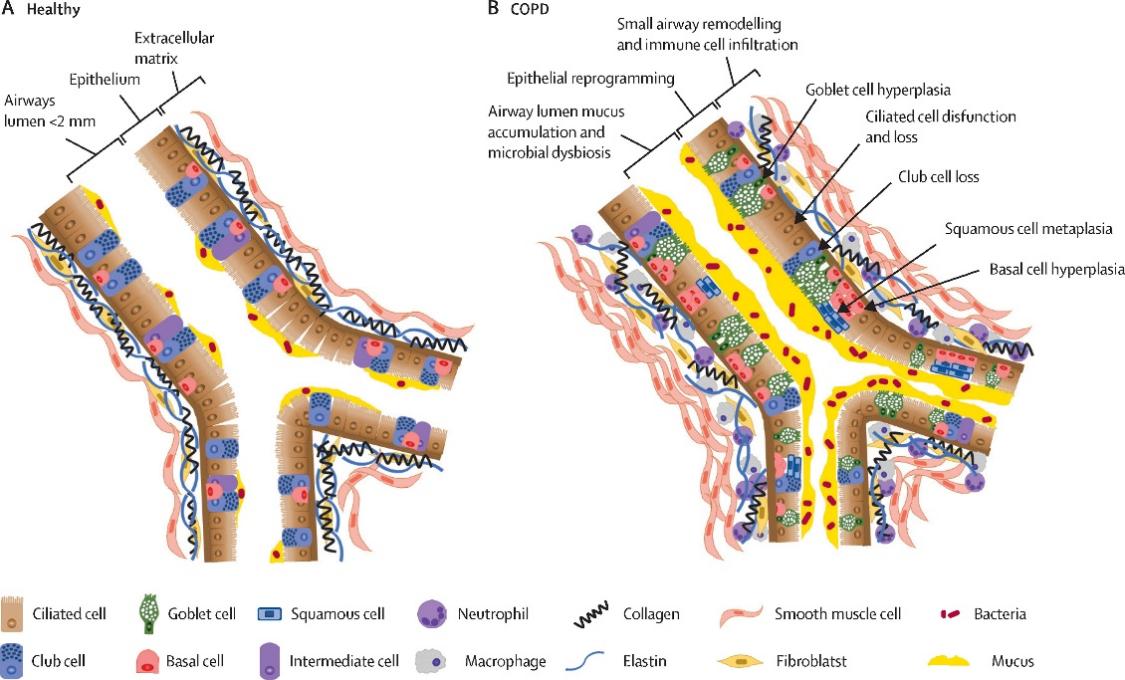
Small airways (<2 mm) are the initial sites of changes in COPD development, including mucus accumulation, immune cell infiltration, and airway wall thickening.
Epithelial reprogramming, combined with immune and remodeling responses, may lead to this progressive reaction and contribute to the development of emphysema.
Macrophages and neutrophils are crucial innate immune cells in the pathogenesis of COPD, associated with chronic inflammation and emphysema progression.
The increased concentration of pathological macrophages in COPD is partially due to oxidative stress-induced resistance to smoking-related apoptosis.
Despite their extended lifespan, COPD-associated macrophages exhibit defective phagocytic function against bacteria and apoptotic cells, leading to increased inflammation.
This defect may be caused by changes in macrophage immunometabolism, including mitochondrial dysfunction and compensatory glycolysis reduction.
Adaptive immune responses and changes in the microbial environment are crucial in COPD. Cell-mediated adaptive immune responses drive inflammation toward four main polarization types:
Type 1 (T1; interferon-driven, typically considered a response to viruses);
Type 2 (T2; driven by IL-4, IL-5, and IL-13, in response to helminths or allergens);
Type 17 (T17; driven by IL-17 and IL-22, responding to extracellular bacteria); and regulatory T cells (Tregs, anti-inflammatory).
Increased T17-driven inflammatory markers in the airways are associated with emphysema, neutrophilic inflammation, and lack of response to inhaled corticosteroids (ICS) [4,5].
Genomic markers of T2 inflammation are associated with elevated eosinophils (one of the primary T2 effector cells) and a better response to ICS [6].
Eosinophil counts were the first blood biomarker added to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines, with evidence suggesting it helps determine the role of ICS in symptomatic patients.
However, anti-IL-5 biologics have not met primary endpoints in COPD trials [7,8].
The limited effectiveness of treating eosinophilic inflammation in COPD alone may be due to overlapping inflammatory changes or irreversible lung damage.
Aging lungs may also be more difficult to treat due to competing pathological alterations, such as stem cell depletion (leading to reduced regenerative capacity) and inflammation [9-11].

As a core tool for simulating the progression of human diseases, verifying drug efficacy, and exploring molecular mechanisms, animal models play a central role in research, and their optimization and application are key steps in promoting clinical translation.
COPD animal models are divided into single-factor induction and multi-factor combined induction models.
Common induction models include cigarette smoke (CS), lipopolysaccharide (LPS), protease, air pollutant-induced models, and gene regulation models.
Multi-factor combined induction models are mainly constructed by combining two or more of the above factors.
Common induction methods include inhalation, nasal drops, intratracheal instillation, and tracheotomy injection, selected according to the different induction factors.
Zvast Biotechnology Model Introduction
Zvast Biotechnology has three COPD models: a mouse COPD model induced solely by smoking, a mouse COPD model induced by smoking combined with LPS, and a rat COPD model induced by smoking combined with LPS.
1. The cigarette smoke-induced COPD model can cause animals to exhibit airway inflammation, increased mucus secretion, and lung tissue damage, which are pathological changes similar to those in human COPD caused by smoking.
2. The model induced by smoking combined with LPS can better simulate the complex pathological process of human COPD.
3. The synergistic effect of LPS and smoking can make lung tissue damage more severe, such as more pronounced pathological changes including alveolar structure destruction, emphysema formation, and interstitial hyperplasia of pulmonary lobules. This is beneficial for studying the mechanisms of lung tissue damage. Moreover, the COPD model induced by smoking alone takes a long time, usually several months, whereas LPS can activate inflammatory cells, accelerating and aggravating pulmonary inflammation and tissue damage, thus effectively shortening the modeling time and improving research efficiency.
By observing the effects of drugs on inflammation, lung function, and lung tissue pathology in the COPD model induced by smoking combined with LPS, the therapeutic efficacy of drugs can be more accurately evaluated.
This helps to reveal the pathogenesis of COPD and the targets for drug treatment, providing a basis for new drug development.