

Aβ pathway faces setbacks, Tau-targeted therapies rise! Gene therapy for Alzheimer disease takes the lead in tackling hard-to-treat populations
When it comes to Alzheimer's disease (AD), the first impression for many might be 'incurable'—after all, this field has been quiet for many years. But recently, top journal *Cell* has been calling out to 'take Tau seriously,' while breakthroughs in gene therapy have also been reported. Has the 'steering wheel' of AD treatment shifted from Aβ to Tau?
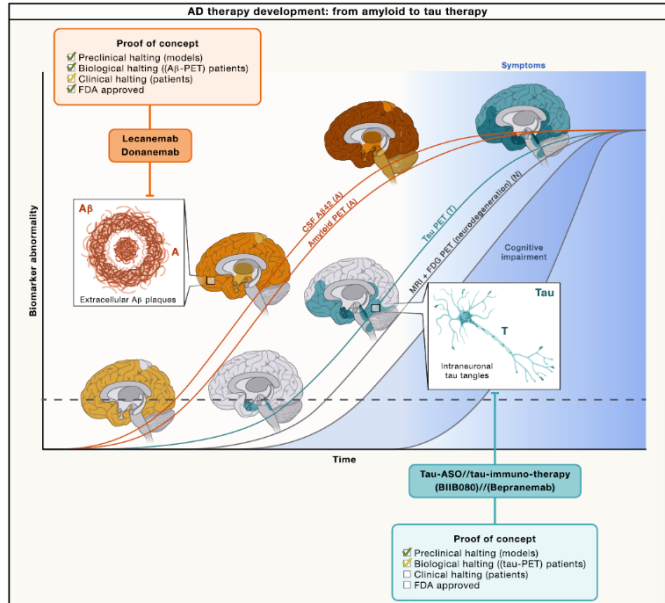
A large amount of clinical data shows that Aβ plaques may begin to accumulate in the brain more than a decade before AD symptoms appear, representing “early presence but temporarily inactive”; whereas neurofibrillary tangles formed by Tau protein have diffusion pathways and deposition rates that almost perfectly align with clinical symptoms such as memory decline, slower reactions, and behavioral abnormalities. Whether through post-mortem pathological analysis, in vivo Tau PET imaging, or measuring Tau protein levels in cerebrospinal fluid, Tau can more accurately explain “why a patient's condition worsens at this stage” than Aβ, serving as a “barometer” of AD progression.
图源:Cell
Major breakthrough! Gene therapy precisely 'targets' high-risk groups
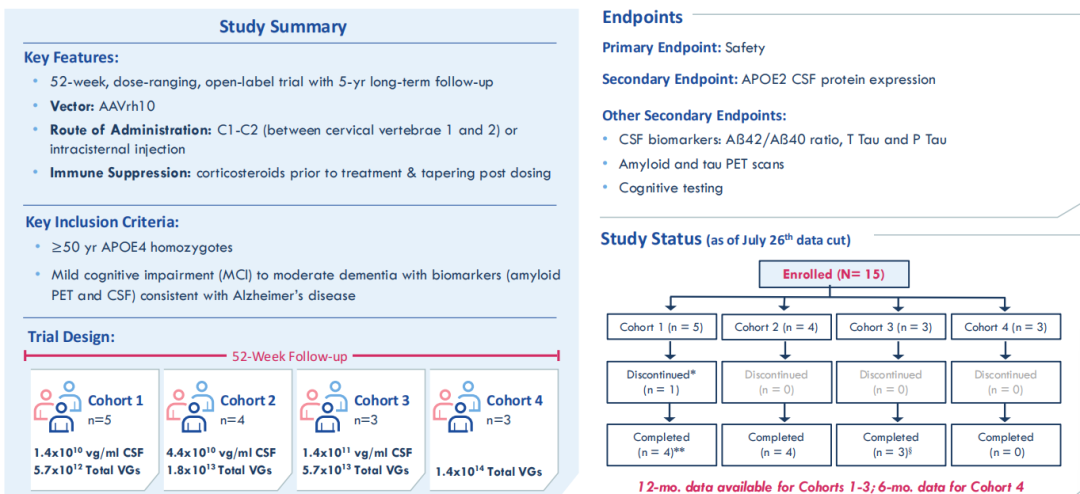
If Tau is the new track, then gene therapy is the 'potential star' on this track. Recently, Lexeo Therapeutics announced its AAV gene therapy LX1001, giving the Alzheimer's disease field a strong boost.
The remarkable aspect of this drug is that it doesn’t cast a wide net; instead, it specifically targets the ‘hard-to-treat population’ of APOE4 homozygotes—people whose risk of developing AD is 12 times higher than average, who account for 15% of all AD cases, and who tend to have early onset, rapid progression, and poor response to previous anti-Aβ drugs.
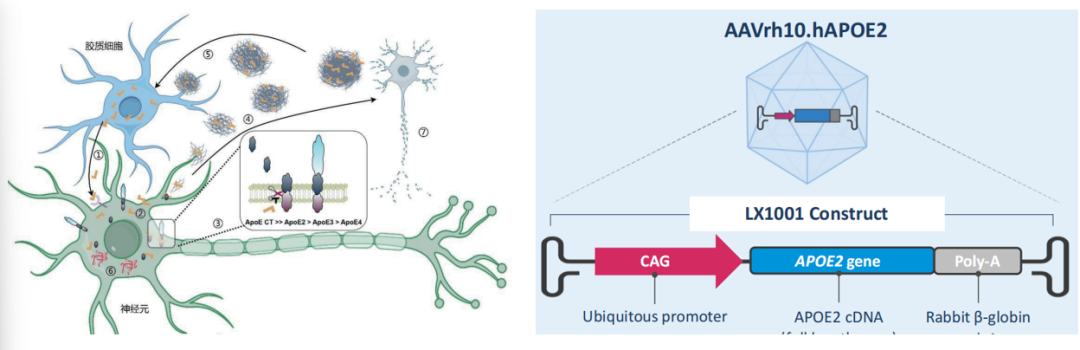
The Role of ApoE in the AD Process & LX1001 Vector Design Image Source: NCT03634007 & GeneFox
What’s even more remarkable is that no common severe side effects of immunotherapy (ARIA) appeared during the 12-month follow-up. It’s worth noting that many AD drugs fail because of side effects, so this balance of 'high efficacy and safety' has everyone looking forward to subsequent clinical trials. Moreover, the latest data for this drug will soon be announced at the JPM Healthcare Conference starting on January 12, when industry leaders from around the world will be paying attention, potentially accelerating the industrialization process of AD therapies.
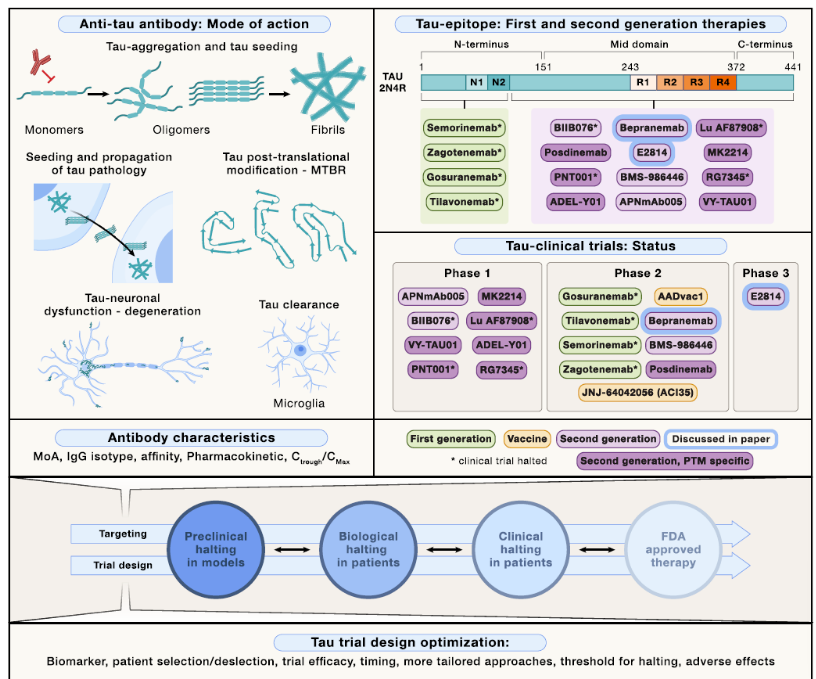
Not just gene therapy, therapies along different technical routes in the Tau-targeted treatment field have shown us the certainty of targeting Tau!
3. Antisense Oligonucleotide BIIB080: This drug takes a “cut off the source” approach—unlike traditional antibodies that "clear already formed Tau proteins," it targets the source directly, using antisense oligonucleotide technology to reduce Tau protein production. In the Phase 1b trial, it already showed a clear dose-dependent effect: the higher the dose, the more significant the reduction in total Tau and phosphorylated Tau in cerebrospinal fluid, and Tau PET imaging also showed a trend of slowed deposition. With this impressive performance, it successfully gained FDA Fast Track designation, essentially receiving a "research acceleration pass," and opened a new direction for Tau-targeted therapy at the "genetic level."
Zvast-Bio Mouse Alzheimer's Disease Model (Double Transgenic)
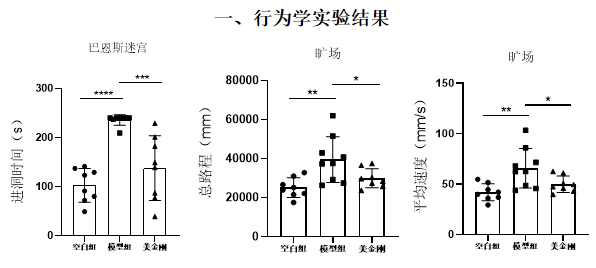
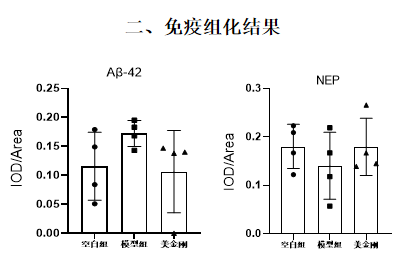
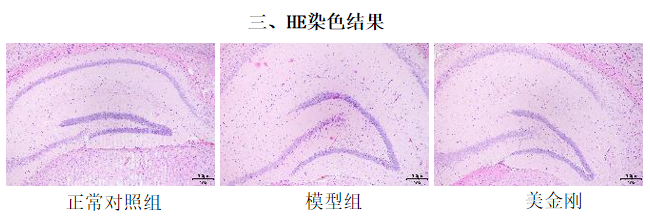
Modeling: APPswe/PS1ΔE9 transgenic mice aged 6-7 months were continued to be raised for 4 weeks, followed by behavioral testing using the Barnes maze and open field test. After testing, brain tissue pathology was examined, as well as the expression of beta-amyloid 42 (Aβ-42) and neprilysin (NEP).
Positive drug: Memantine hydrochloride tablets, administered by gavage, once per animal per day, administered continuously for 5 weeks.
Positive drug: Memantine hydrochloride tablets, administered by gavage, once per animal per day, administered continuously for 5 weeks.