From Anti-Inflammation to Precision Targeting: Pericarditis Treatment Enters the Era of Individualized Medicine
The heart is tightly encased in a "constrictive sac" filled with inflammatory fluid, and every heartbeat is accompanied by knife-like pain. This is not an exaggeration, but the daily reality for millions of patients with recurrent pericarditis.
Once, "anti-inflammation" was the core goal of pericarditis treatment, with doctors relying on broad-spectrum anti-inflammatory drugs to relieve symptoms. Today, driven by in-depth decoding of disease mechanisms and the iterative upgrading of targeted therapies, pericarditis treatment has entered a new era of "precision targeting + individualized stratification," bringing new hope to patients for saying goodbye to recurrent pain.
Pericarditis: A Cardiovascular Inflammation That Cannot Be Ignored
Pericarditis is a common disease in the cardiovascular field, referring to inflammation of the pericardium (the fibrous serosal sac enclosing the heart) caused by factors such as infection, immune response, and trauma. Its core pathological manifestations include pericardial hyperemia, edema, and inflammatory cell infiltration. In severe cases, pericardial effusion, adhesion, and thickening may occur, and the condition can even progress to constrictive pericarditis, thereby impairing cardiac diastolic function.
According to the duration of the disease, it can be classified into three types: acute pericarditis (duration <6 weeks), subacute pericarditis (duration 6 weeks–3 months), and chronic pericarditis (duration> 3 months). In terms of disease prevalence, acute pericarditis accounts for approximately 0.2% of cardiovascular inpatients worldwide. In China, there are over 80,000 new cases of pericarditis each year, showing an increasing trend year by year. This disease has become a non-negligible burden on cardiovascular health.
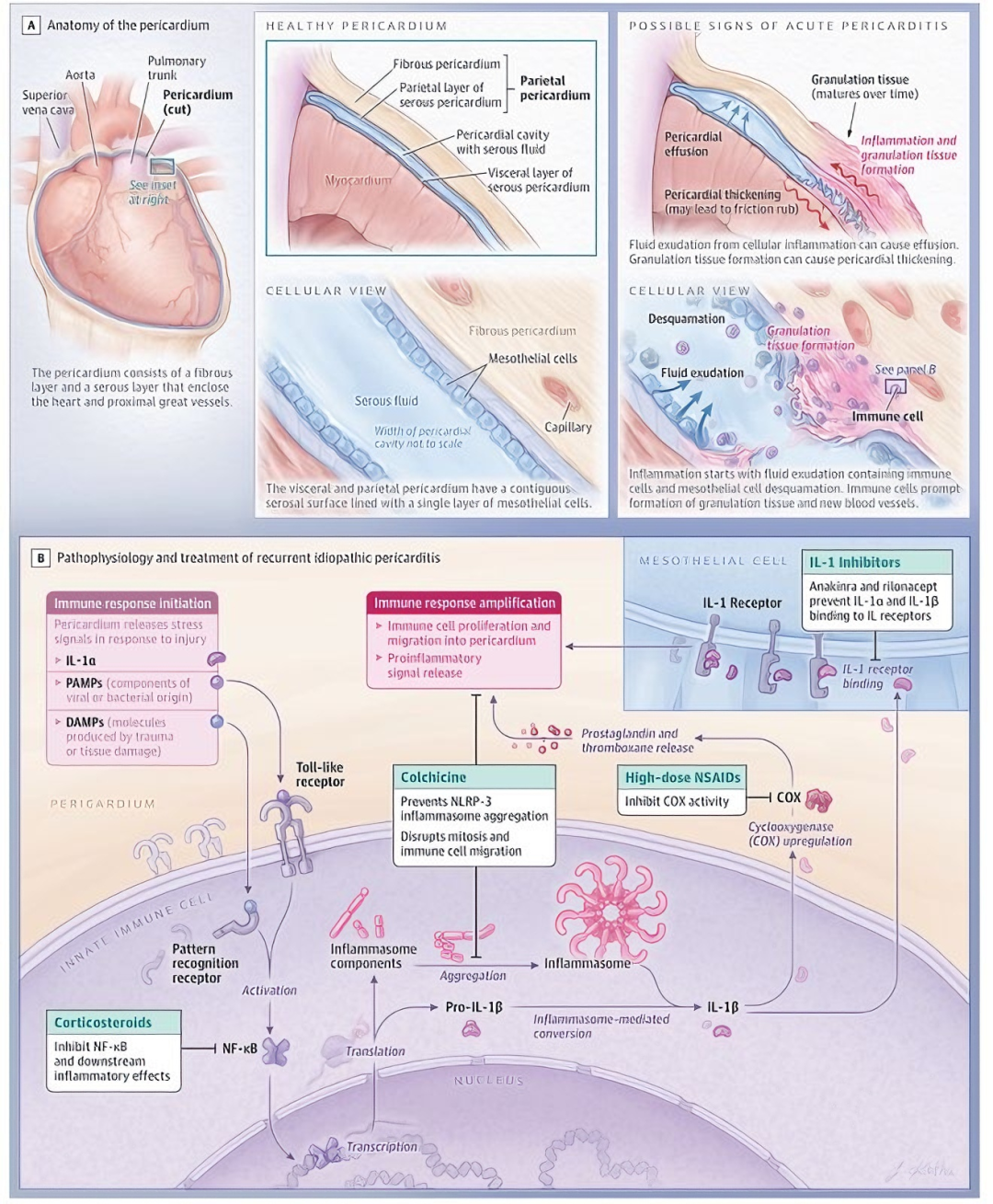
Image Source: JAMA
Exploring the Pathogenesis
Tracing back to its origins, the core pathogenesis of pericarditis lies in the abnormal activation of inflammatory signaling pathways and subsequent tissue damage in the pericardium following pathogen invasion, autoimmune attack, or physicochemical stimulation. Mechanisms vary significantly by etiology, which can be specifically categorized into two types:
(1)Infectious mechanisms: Viruses can directly invade pericardial tissue or induce inflammation through immune complex deposition (e.g., post-infection CD4+ T cell infiltration and release of pro-inflammatory cytokines such as IL-6 and TNF-α). Bacteria and Mycobacterium tuberculosis spread via hematogenous dissemination or adjacent tissue extension, causing suppurative and tuberculous pericarditis, respectively.
(2)Non-infectious mechanisms: Mostly associated with immune abnormalities. For example, autoimmune diseases like systemic lupus erythematosus (SLE) attack pericardial antigens through cross-immune reactions; alternatively, myocardial necrosis following acute myocardial infarction releases self-antigens, inducing delayed immune-mediated pericarditis.
IL-1 Inhibitors: A Precision Therapeutic Tool
Before the era of individualized treatment, pericarditis management remained stuck in the phase of "empirical anti-inflammation" for a long time. Conventional first-line regimens (non-steroidal anti-inflammatory drugs + colchicine) are effective for most acute patients, but approximately 15%-30% of patients face the dilemma of disease recurrence after drug withdrawal. Research ultimately revealed that the core crux of this predicament lies in the persistent abnormal activation of the interleukin-1 (IL-1) inflammatory pathway—simple broad-spectrum anti-inflammation cannot block this pathological process at its root.
Although early IL-1 inhibitors represented by anakinra achieved precise blocking of the inflammatory pathway and broke the limitations of traditional treatment, the frequent administration via daily injections severely compromised patients’ long-term treatment adherence and efficacy stability, becoming a "stumbling block" on the path to precision therapy.
In 2025, the ACC and ESC updated their guidelines, officially advancing pericarditis diagnosis and treatment into the era of individualized care—marking a critical turning point in the revolution from "anti-inflammation" to "precision targeting." The core innovation of the new guidelines is that treatment decisions are no longer a "one-size-fits-all" approach but are stratified and driven based on the precise assessment of patients’ inflammatory phenotypes. For patients with "inflammatory phenotypes" unresponsive to first-line therapy, targeted anti-IL-1 agents have been established as the preferred regimen, signifying the official transition of pericarditis treatment from traditional broad-spectrum anti-inflammation to a new phase of precise immunomodulation.
Image Source: ACC Guidelines
Image Source: ESC Guidelines
Medical exploration never ceases. Next-generation interleukin-1 (IL-1) inhibitors are advancing rapidly toward the goals of “higher specificity, longer half-life, and lower infection risk.” For example, DNL659, developed by Denali Therapeutics, can precisely target its intended molecule while sparing “innocent” components like IL-1β that mediate normal immune function. This not only potently suppresses pathological inflammation but also significantly reduces the patient’s risk of infection, thereby greatly expanding the therapeutic safety window.
Precision Targeted Therapy Holds Great Promise for the Future
In the future, with the popularization of gene sequencing and biomarker detection, physicians will even be able to predict which IL-1 inhibitor a patient will respond to best before treatment initiation. The "arsenal" of targeted therapies is constantly expanding, and pericarditis—an ancient disease—is being redefined by modern medicine. For countless patients enduring recurrent chest pain, a future free from recurrence and filled with peace of mind is becoming clearer than ever before. Moreover, this revolution from "empirical anti-inflammation" to "precision targeting" signifies that the treatment of cardiovascular diseases has entered a more precise, safer era of individualized medicine.
Zvast Bio Pericarditis Model
Alc-induced Aseptic Pericarditis Model in Rats
Animals: Sprague-Dawley (SD) Rats
Groups:
1) Sham Operation Group (N=9);
2) Model Group (N=9);
3) Model + Colchicine Group (N=9)
Modeling: Injection of talc suspension between the pericardium and myocardium of rats
Positive Control: Colchicine
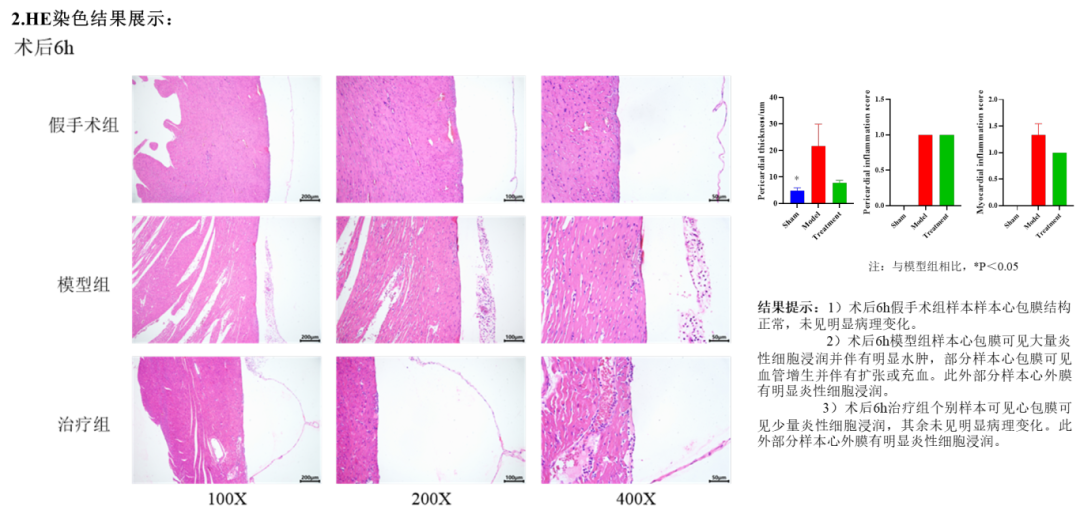
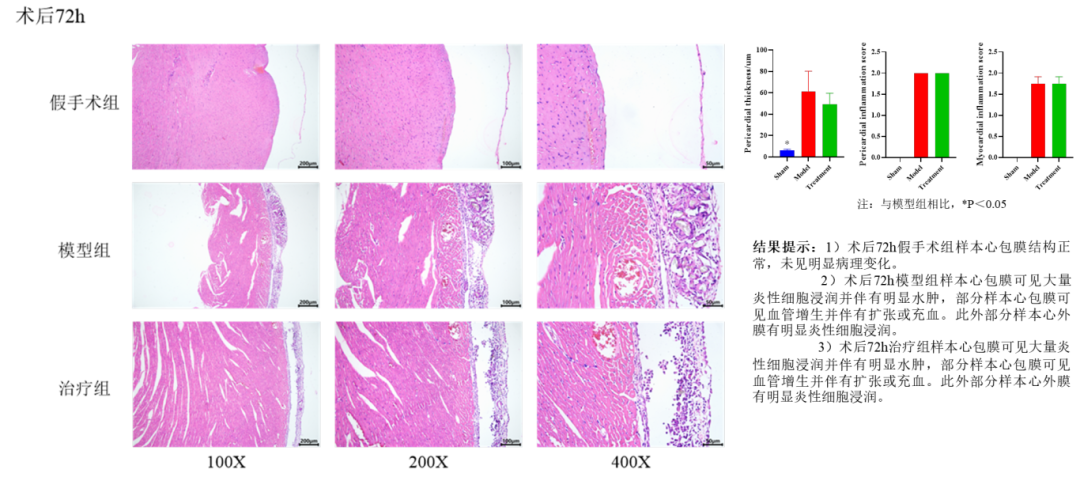
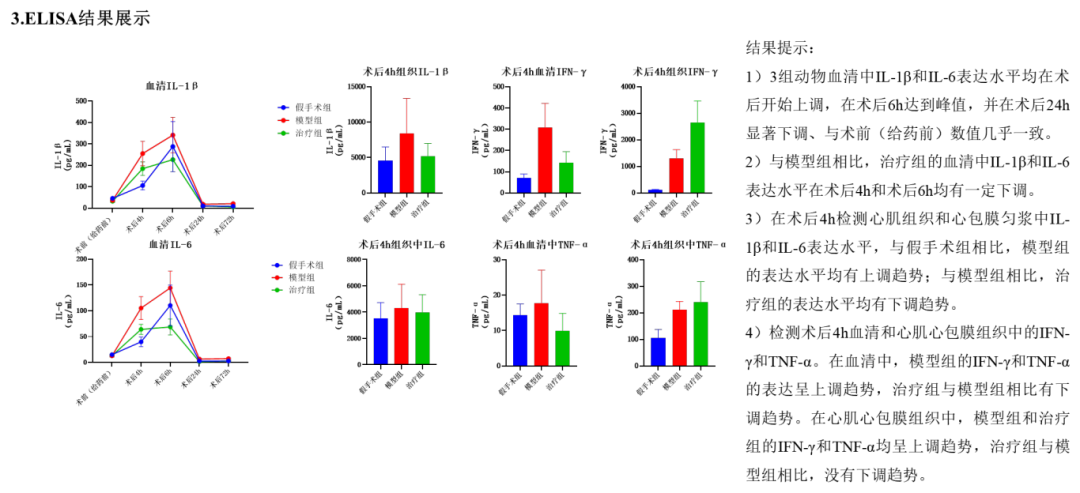
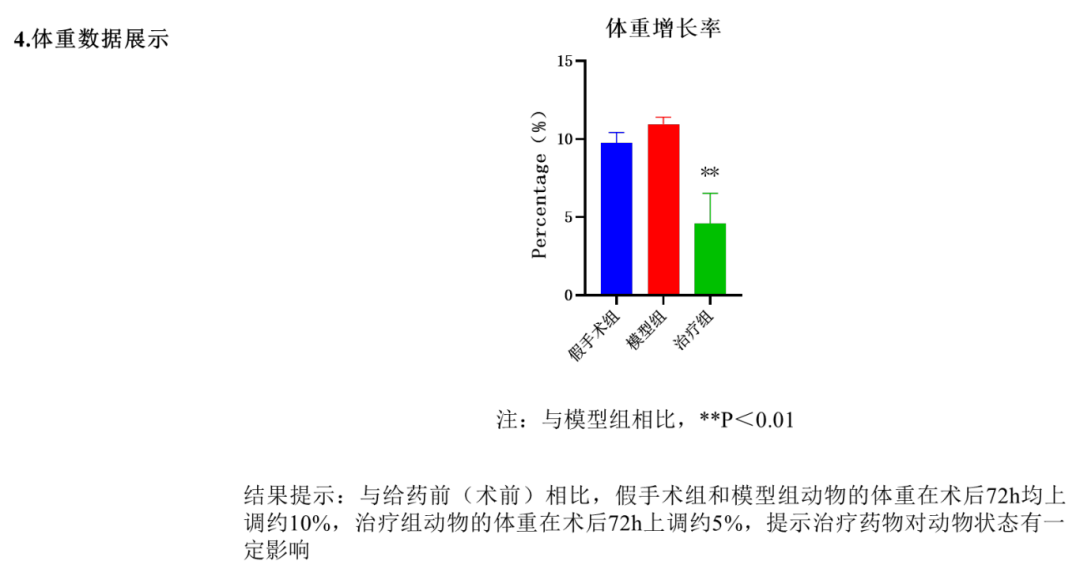
Result: